A digital guided self-help course to treat depression in India, all on WhatsApp
people treated to date
people currently in the programme
$24
cost to treat someone for depression in April
life satisfaction point increase per person
Depression is widespread in India, and getting worse
67 million
Indians suffer from depression each year
85%
don't get any treatment at all
1 in 3
global female suicides take place in India
In India, 67 million people experience a depressive episode every year, 4.7 million self-harm, and 200,000 die by suicide.[1][2][3] More than one in three of the world's female suicides take place in India.[4][5] And while only 2.6% of the population had depression three decades ago, it's increased by nearly half to 4% today.[6]
But despite the scope of the problem, 85% of Indians with depression receive no treatment whatsoever.[7]
Low-cost, scalable solutions are needed
28¢
federal spending per mentally ill person
50×
less mental health workers than the global median in the poorest states
two‑fifths
of average weekly pay for casual workers to afford therapy
That's because there aren't enough resources invested in mental health. The federal government only spends 28 US cents per mentally ill person each year on care, or 0.5% of the total health budget.[8] State spending isn't routinely reported and is likely negligible in the poorest states.
These states—typically northern, typically Hindi-speaking—have around 1 public sector mental health worker per million people.[9] That's around 20× less than other low–middle income countries (LMICs), and 50× less than the global median.[10] Bihar, a state the size of Japan, only has 7 government-registered psychologists and spends less than a cent per mentally ill person on the government's primary care programme for mental health.[11][12]
With such low supply, therapy has become a luxury. A typical session costs ₹1,000, or two-fifths of a week's pay for a casual labourer.[13][14] Any serious intervention needs to massively increase the number of workers to cover the front lines of care, freeing up the remaining workforce to tackle more serious cases.
Kaya Guides is the world's first non-profit to implement WHO's guided self-help programme
Guided self-help is a well-known technique in the academic literature that blends self-help with real human support, focused on agency and resilience.
Kaya Guides builds on decades of evidence by adapting WHO's flagship guided self-help programme, Step-by-Step, to digital platforms people check hundreds of times a day.[15] Participants find our WhatsApp bot when they're scrolling social media—usually late at night, outside of typical service hours, in the middle of an episode.[16]

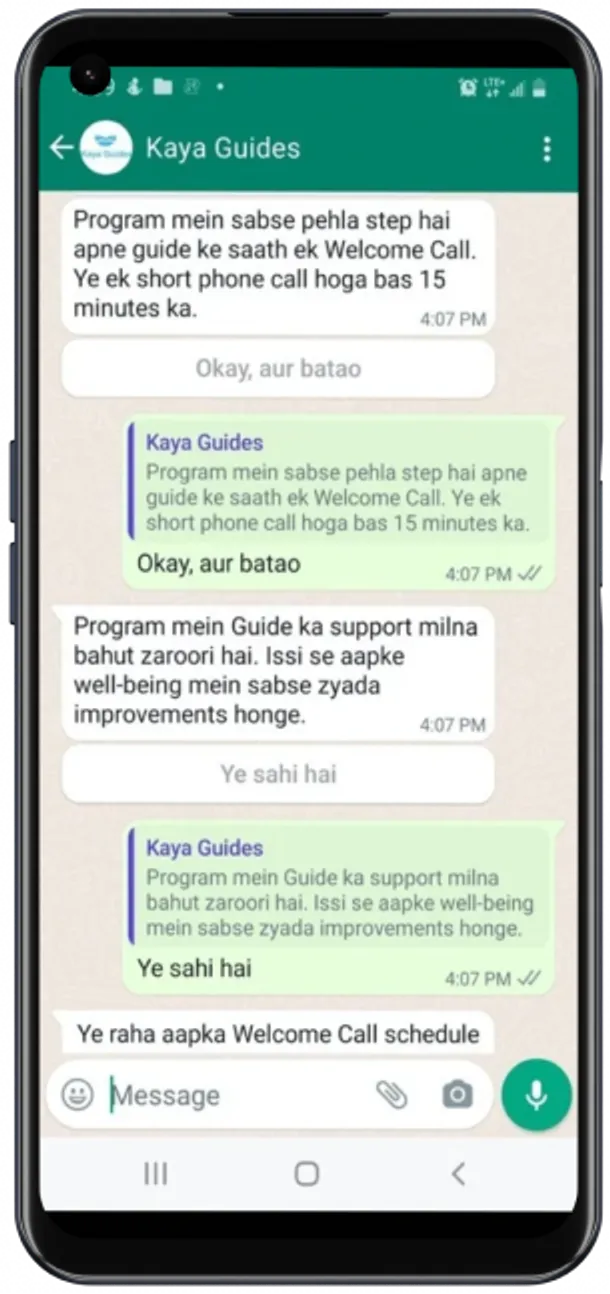


Over the next 8 weeks, they learn evidence-based emotional regulation and coping techniques. Lay counsellors then help them adapt these techniques to their problems in rapid, 15-minute sessions. Once they can self-regulate, they recover the agency to pursue longer-term solutions to their problems, like leaving abusive family environments, rejoining their jobs, or applying for college.
"Since my marriage, I've had three abortions. I grew up in a violent household and now face abuse from my partner and in-laws. These calls are my only support system."
—25-year-old, Rajasthan
A meta-analysis of more than 15,000 participants was unable to find a difference in effectiveness between guided self-help and traditional individual or group therapy; but did find that adding human counsellors significantly increased effectiveness.[18] Another meta-analysis (8,107 participants) found significant improvements in engagement from adding human support.[19] There is no evidence that stronger qualifications improve effectiveness or engagement, such that lay mental health workers are highly effective and even non-inferior to accredited psychotherapists in large trials for treating common mental illnesses.[20][21][22]
…and our results follow WHO's closely
Step-by-Step showed moderate to large effects in reducing depression in all three of WHO's RCTs.[23][24][25] The programme was designed to be highly adaptable,[26][27][28][29] and is currently being implemented in Lebanon,[23:1][24:1][25:1] China,[30][31][32] Egypt,[33][34] Switzerland,[35][36] Germany,[34:1][35:1][36:1] Thailand,[37] Zambia,[38] Sweden,[34:2] and Macao.[39]
Our results follow theirs closely. Over
It's not empty engagement, either. Our participants complete
In 2026, we're running an RCT to further validate our results against a control group.
We're growing
We're young, but moving fast. In 2023, our pilot treated
In April, it cost us ~$24 to treat someone for depression. But at scale, our cost structure will get it down to $9[42]. Compared to other leading mental health charities, we've reached comparable cost-effectiveness in less than a third of the time, and are ≥2× cheaper than they were at the same scale.
If you can help us get there, reach out! We'd love to hear from you.
For donations above $1,000, please get in touch directly
Global Burden of Disease Collaborative Network (2023) Global Burden of Disease Study 2023, Seattle, United States: Institute for Health Metrics and Evaluation (IHME). ↩︎
Hay, Simon I. et al. (2025) Burden of 375 diseases and injuries, risk-attributable burden of 88 risk factors, and healthy life expectancy in 204 countries and territories, including 660 subnational locations, 1990–2023: a systematic analysis for the Global Burden of Disease Study 2023, The Lancet, vol. 406, pp. 1873–1922. ↩︎
Naghavi, Mohsen et al. (2025) Global burden of 292 causes of death in 204 countries and territories and 660 subnational locations, 1990–2023: a systematic analysis for the Global Burden of Disease Study 2023, The Lancet, vol. 406, pp. 1811–1872. ↩︎
Dandona, Rakhi et al. (2018) Gender differentials and state variations in suicide deaths in India: the Global Burden of Disease Study 1990–2016, The Lancet Public Health, vol. 3, pp. e478–e489. ↩︎
Global Burden of Disease Collaborative Network (2023) Global Burden of Disease Study 2023, Seattle, United States: Institute for Health Metrics and Evaluation (IHME). ↩︎
Global Burden of Disease Collaborative Network (2023) Global Burden of Disease Study 2023, Seattle, United States: Institute for Health Metrics and Evaluation (IHME). ↩︎
Gururaj, G et al. (2016) National Mental Health Survey of India, 2015–16: Prevalence, Patterns, and Outcomes, Bengaluru: National Institute of Mental Health and Neuro Sciences. Although this report is from 2016, newer global estimates of service coverage suggest the trend is stable. See Santomauro, Damian F. et al. (2024) Service coverage for major depressive disorder: estimated rates of minimally adequate treatment for 204 countries and territories in 2021, The Lancet Psychiatry, vol. 11, pp. 1012–1021. ↩︎
India Mental Health Observatory (2026) Budget for Mental Health - Analysis of Union Budget 2026–2027, Keshav Desiraju / India Mental Health Observatory. Care amounts are calculated by excluding NIMHANS, LGBRIMH, and CIP, which are primarily research hospitals. The total mentally ill population was computed from Global Burden of Disease Collaborative Network (2023) Global Burden of Disease Study 2023, Seattle, United States: Institute for Health Metrics and Evaluation (IHME). ↩︎
Gururaj, G et al. (2016) National Mental Health Survey of India, 2015–16: Mental Health Systems, Bengaluru: National Institute of Mental Health and Neuro Sciences. ↩︎
World Health Organization (2018) Mental Health Atlas 2017, Geneva, Switzerland. Although newer data was available, this was chosen to temporally match India's most recent data from 2016. ↩︎
Unstarred Question No. 1408: Mental Illness, (2023) Government of India, Ministry of Health and Family Welfare, Department of Health and Family Welfare. ↩︎
Unstarred Question No. 288: Budgetary Allocations for Mental Health Care, (2025) Government of India, Ministry of Health and Family Welfare, Department of Health and Family Welfare. The total mentally ill population was computed from Global Burden of Disease Collaborative Network (2023) Global Burden of Disease Study 2023, Seattle, United States: Institute for Health Metrics and Evaluation (IHME). ↩︎
Kumar, CTL Kiran et al. (2024) Health insurance for psychotherapy in India, Indian Journal of Psychiatry, vol. 66, pp. 466–471. ↩︎
Government of India, Ministry of Statistics and Programme Implementation, National Statistics Office (2026) Period Labour Force Survey (PLFS) (January–December 2025). Casual weekly pay is calculated by multiplying the daily rate by 6 days—true average wages are probably less. ↩︎
Carswell, Kenneth et al. (2018) Step-by-Step: a new WHO digital mental health intervention for depression, mHealth, vol. 4, pp. 34–34. ↩︎
% of new participants join after 9pm and before 9am, peaking between 12–1am. The average new participant scores points on the PHQ-9, 1.3 points above WHO's Step-by-Step RCTs, where it was 16.4. ↩︎ In the last 90 days,
% received their first call within 24 hours of their first message, and an additional % in the following 24 hours. When signing up for the programme, participants are invited to book a call within the following 7 days; these statistics exclude people who booked but never accepted a call, and excludes call attempts which didn't result in a completed session. ↩︎ Cuijpers, Pim et al. (2019) Effectiveness and Acceptability of Cognitive Behavior Therapy Delivery Formats in Adults With Depression: A Network Meta-analysis, JAMA Psychiatry, vol. 76, p. 700. ↩︎
Karyotaki, Eirini et al. (2021) Internet-Based Cognitive Behavioral Therapy for Depression: A Systematic Review and Individual Patient Data Network Meta-analysis, JAMA Psychiatry, vol. 78, p. 361. ↩︎
Leung, Calista et al. (2022) The Effects of Nonclinician Guidance on Effectiveness and Process Outcomes in Digital Mental Health Interventions: Systematic Review and Meta-analysis, Journal of Medical Internet Research, vol. 24, p. e36004. ↩︎
Koelen, J. A. et al. (2022) Man vs. machine: A meta-analysis on the added value of human support in text-based internet treatments ("e-therapy") for mental disorders, Clinical Psychology Review, vol. 96, p. 102179. ↩︎
Richards, David A. et al. (2016) Cost and Outcome of Behavioural Activation versus Cognitive Behavioural Therapy for Depression (COBRA): a randomised, controlled, non-inferiority trial, The Lancet, vol. 388, pp. 871–880. ↩︎
Cuijpers, Pim et al. (2022) Effects of a WHO-guided digital health intervention for depression in Syrian refugees in Lebanon: A randomized controlled trial, PLOS Medicine, vol. 19, p. e1004025. ↩︎ ↩︎
Cuijpers, Pim et al. (2022) Guided digital health intervention for depression in Lebanon: randomised trial, Evidence Based Mental Health, vol. 25, pp. e34–e40. ↩︎ ↩︎
Heim, Eva et al. (2021) Step-by-step: Feasibility randomised controlled trial of a mobile-based intervention for depression among populations affected by adversity in Lebanon, Internet Interventions, vol. 24, p. 100380. ↩︎ ↩︎
Sijbrandij, Marit et al. (2017) Strengthening mental health care systems for Syrian refugees in Europe and the Middle East: integrating scalable psychological interventions in eight countries, European Journal of Psychotraumatology, vol. 8, p. 1388102. ↩︎
Burchert, Sebastian et al. (2019) User-Centered App Adaptation of a Low-Intensity E-Mental Health Intervention for Syrian Refugees, Frontiers in Psychiatry, vol. 9, p. 663. ↩︎
Abi Ramia, J. et al. (2018) Community cognitive interviewing to inform local adaptations of an e-mental health intervention in Lebanon, Global Mental Health, vol. 5, p. e39. ↩︎
Woodward, Aniek et al. (2023) Scalability of digital psychological innovations for refugees: A comparative analysis in Egypt, Germany, and Sweden, SSM - Mental Health, vol. 4, p. 100231. ↩︎
Li, Gen et al. (2024) A WHO digital intervention to address depression among young Chinese adults: a type 1 effectiveness-implementation randomized controlled trial, Translational Psychiatry, vol. 14, p. 102. ↩︎
Sit, Hao Fong et al. (2021) A Feasibility Study of the WHO Digital Mental Health Intervention Step-by-Step to Address Depression Among Chinese Young Adults, Frontiers in Psychiatry, vol. 12, p. 812667. ↩︎
Sit, Hao Fong et al. (2020) The Cultural Adaptation of Step-by-Step: An Intervention to Address Depression Among Chinese Young Adults, Frontiers in Psychiatry, vol. 11, p. 650. ↩︎
Burchert, Sebastian et al. (2024) Effects of a self-guided digital mental health self-help intervention for Syrian refugees in Egypt: A pragmatic randomized controlled trial, PLoS Medicine, vol. 21, p. e1004460. ↩︎
Woodward, Aniek et al. (2023) Scalability of digital psychological innovations for refugees: A comparative analysis in Egypt, Germany, and Sweden, SSM - Mental Health, vol. 4, p. 100231. ↩︎ ↩︎ ↩︎
Heim, Eva et al. (2024) Effect of Cultural Adaptation of a Smartphone-Based Self-Help Programme on Its Acceptability and Efficacy: Randomized Controlled Trial, Clinical Psychology in Europe, vol. 6, pp. 1–23. ↩︎ ↩︎
Heim, Eva et al. (2024) Why Did Our Trial Not Work Out? A Qualitative Analysis, Clinical Psychology in Europe, vol. 6, p. e12887. ↩︎ ↩︎
World Health Organization (2025) Thailand adapts WHO's Step-by-Step programme as part of national digital mental health platform, May 20. ↩︎
Clare, Abbie et al. (2025) Adapting WHO's Step-By-Step Digital Intervention for Anxiety and Depression for Delivery Via Radio: Development, Piloting and Mixed-Methods Evaluation of the Lumuno Radio Campaign In Zambia, Mental Health Science, vol. 3, p. e70035. ↩︎
Garabiles, Melissa R. et al. (2019) Exploring comorbidity between anxiety and depression among migrant Filipino domestic workers: A network approach, Journal of Affective Disorders, vol. 250, pp. 85–93. ↩︎
In the past year,
out of participants ( %) completed the programme and the post-treatment survey, reporting the results in this section. Although this rate is somewhat low, participants tend to complete the post-treatment survey at representative rates of programme engagement, as the post-treatment survey is offered to all participants at 8 weeks regardless of progress. ↩︎ Helliwell, John F. et al. (2026) World Happiness Report 2026, University of Oxford: Wellbeing Research Centre. ↩︎
We report our costs in terms of total costs per participant, while fully accounting for partnerships—this is the least charitable accounting of our costs. It can be hard to compare between charities, as some exclude the costs of partnerships, and others exclude all overhead costs entirely. ↩︎